Pressure on Healthcare Systems: Coping with Demand for ICU and Hospital Beds
The rapid spread of the virus and the special care that critical patients need put a major pressure on the European healthcare system. Not every European country was adequately prepared to handle this crisis.
Over the last past months, it has become clear that the Coronavirus poses a considerable health threat on a global scale. The virus that causes the illness COVID-19 is called the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). The virus mainly attacks healthy cells located in the lungs, causing respiratory problems. To alleviate the breathing difficulties in the most serious cases, a ventilator is used to push air, with increased levels of oxygen, into the lungs. While most of the infected patients experience minor flu-related symptoms, up to 20% of the cases require hospitalisation. Exact rates differ per country, though approximately 5-8% of the infected population need intensive care unit (ICU) admission, which lasts an average of 3-4 weeks. The rapid spread of the virus, especially before the lockdown measures were implemented, put major pressure on the healthcare systems in some European countries.
With this data story we would like to give a big shout-out to all the healthcare workers who continue to work and help those in need during this pandemic. These hard workers must cope with scarce resources, endure long hours, and face dangerous situations. We would not be able to manage this crisis without them.
Preparing for COVID-19: Pre-crisis situation
Leading up to the Coronavirus outbreak, countries investigated whether their healthcare systems were adequately prepared for a pandemic. Last year, the Global Health Security Index (also discussed in a previous data story) was established, which is a comprehensive assessment of the preparation of for epidemics and pandemics for 195 countries. The index concluded in October 2019, that collectively, international capacity for preventing, detecting, and responding to pandemics was very weak. For example, there are many countries that received a low score on national public health emergency preparedness and response plan, emergency response operations, linking public health and security authorities, and systems in place for dispensing medical countermeasures during a public health emergency.
One way to assess the preparedness of different countries to tackle COVID-19, is to look at the number of hospital beds per country. Open data on intensive care beds is scarce, but on average between 2010 and 2011, European countries had 11.5 critical care beds per 100,000 inhabitants. This number fluctuates between countries. For example, Germany reported 29.2 beds per 100,000 inhabitants whereas Portugal reported 4.2. A broader, and more recent, perspective is provided when looking at acute care hospital beds – acute care largely depends on time-sensitive and rapid intervention and extends beyond the intensive care unit. Using data from 2014, gathered by the World Health Organization (WHO), figure 1 was created, showing the number of acute care hospital beds per 100,000 inhabitants per country. It can be seen that, on average, EU Member States have 394 hospital beds for acute care available per 100,000 inhabitants.
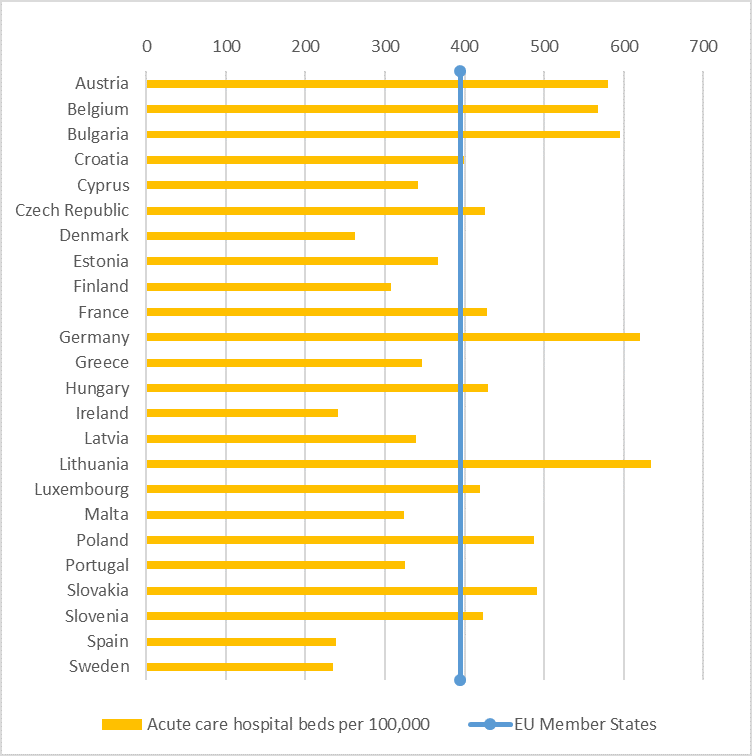
Figure 1: Number of acute care hospital beds per 100,000 inhabitants in 2014, source: WHO
Flattening the curve
In the early weeks of the outbreak, Italy reported an exponential increase in the number of infected people which doubled every 2-4 days. At the peak of the crisis, physicians had to make wrenching triage choices and only help those with a reasonable chance of survival, sometimes being obliged to leave older patients to die alone in their houses without appropriate care. The explosive rate at which the virus had spread in Italy also raised the question in other countries whether there were enough hospital beds, doctors, and resources available to treat all the infected patients with severe symptoms. As a response, governments implemented restrictive measures to lower the spread of the virus. This strategy is often referred to as ‘flattening the curve’, which is visualised in figure 2.
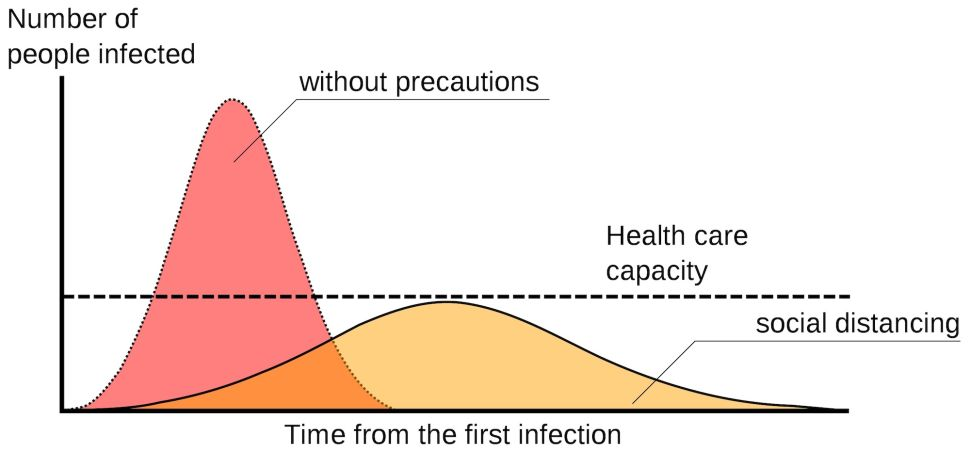
Figure 2: Visualisation of ‘flattening the curve’, source: live science.
The faster the infection curve rises, the higher the maximum amount of infections will be at the peak. Healthcare systems have limitations on patient handling capacity, as discussed earlier, and are not equipped to handle large infection peaks. These systems can get overwhelmed quickly if the curve is not controlled or flattened.
When social distancing was implemented in society, the infection rate was expected to subside leading to a flattening of the curve. By spreading the cases over time, the pressure on the healthcare system can be eased up thus allowing them to administer better care and potentially prevent many deaths. To visualise how countries are flattening the curve, the Johns Hopkins University (JHU) mapped the 5-day moving averages of daily infected people for the 10 most affected countries, see figure 3.
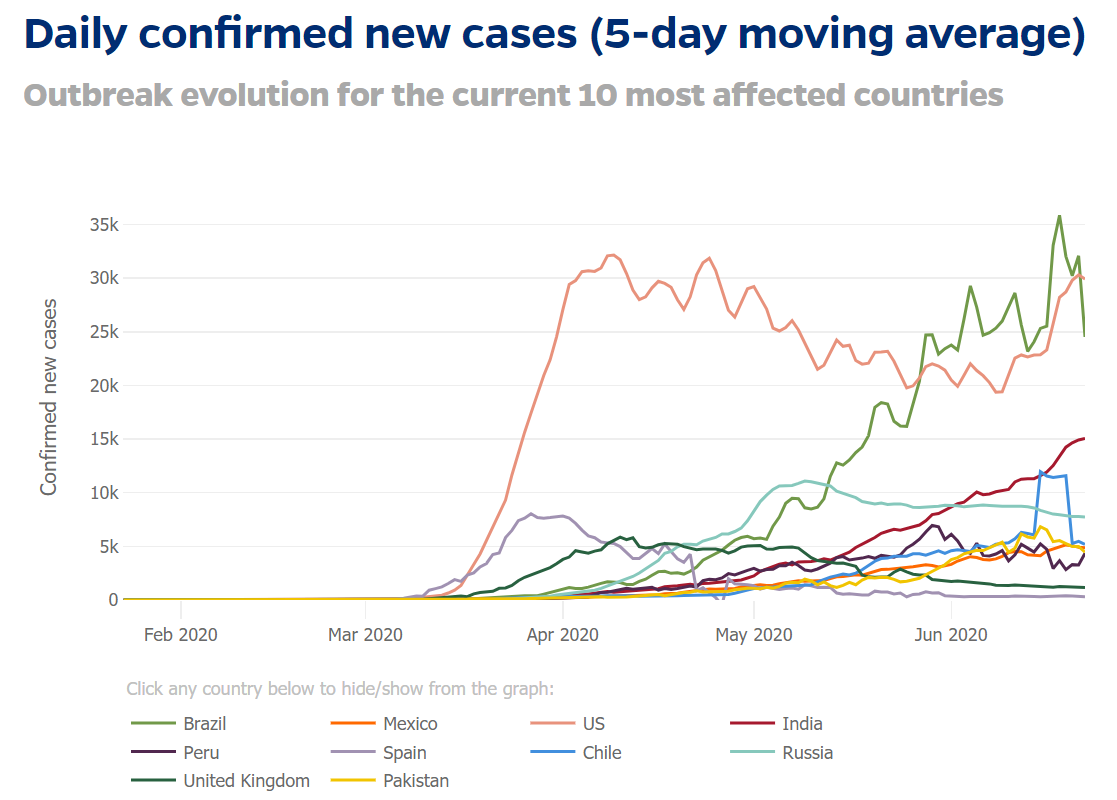
Figure 3: Visualisation created by Johns Hopkins University on daily confirmed cases for 10 most affected countries.
Demand for hospital and ICU beds during COVID-19
In order to monitor the pressure on healthcare systems, it is important to closely follow the demand for hospital and ICU beds. Several countries published national data about the demand and availability of hospital beds, for example Austria, Spain, Italy, France, and Germany.
The Institute for Health Metrics and Evaluation (IHME) is an independent global health research centre at the University of Washington that publishes data related to COVID-19. The European Data Portal used data from IHME to create an interactive visualisation on the demand for hospital beds per available European country, shown in figure 4. Per country, the total number of ICU beds, the number of ICU beds occupied per day with COVID-19 patients, the number of ICU beds occupied with COVID-19 patients added to the pre-crisis average of occupied ICU beds per day, and the number of normal hospital beds occupied per day for COVID-19 patients are illustrated. It provides an overview of which countries exceeded their maximum ICU bed capacity during the last few months.
It should be noted that several countries implemented measures to lower the demand of ICU beds for non-COVID-19 patients by, for example, postponing surgeries. Also, the restrictions on travelling and mobility led to fewer accidents. This can influence the need for ICU beds per day in general, not just for COVID-19 patients.
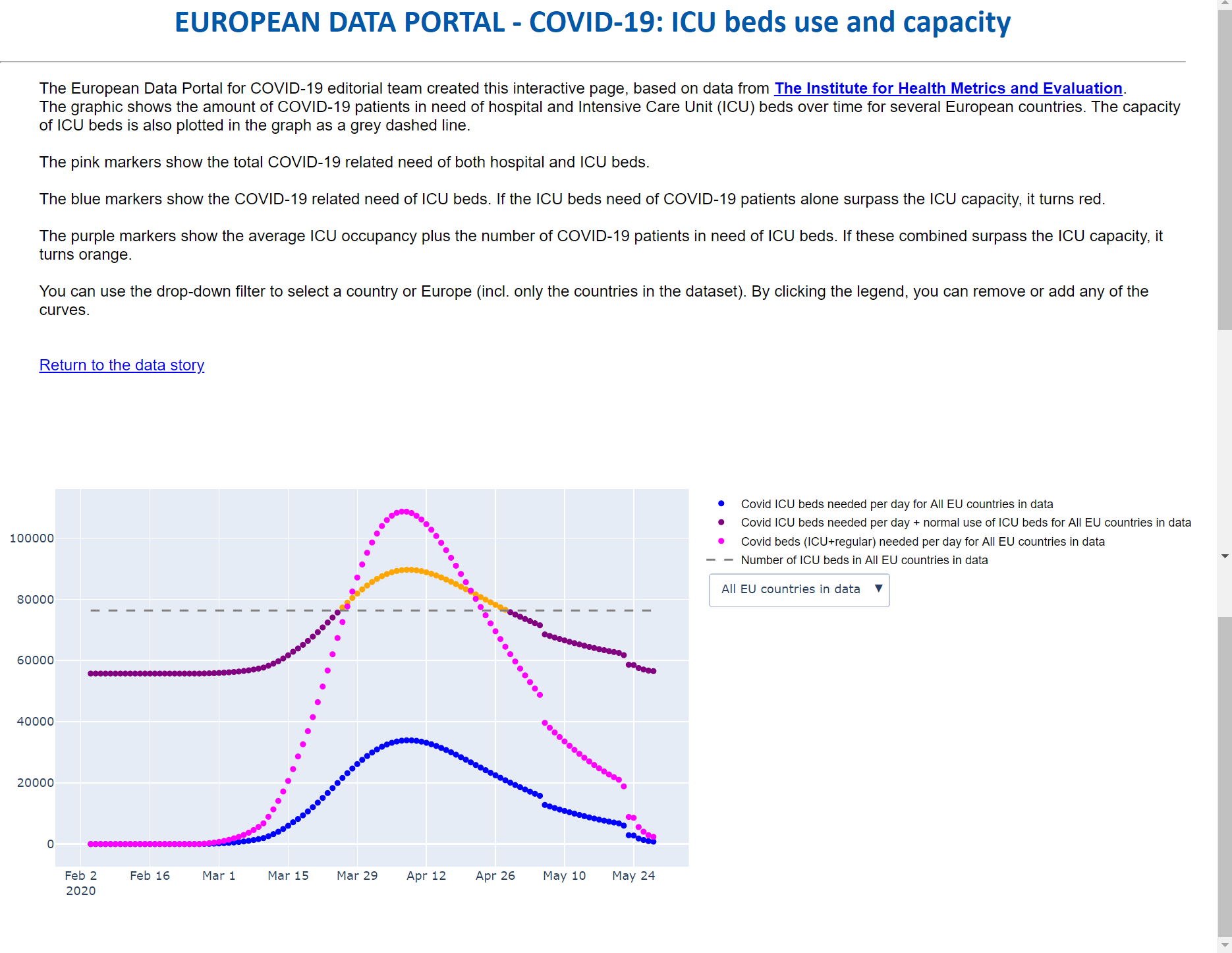
Figure 4: Screenshot of interactive visualisation on demand of hospital bed for COVID-19 patients, source: IHME.
As the number of infected people steeply increased, the demand for hospital and ICU bed also grew rapidly. The preparedness in terms of hospital beds, skilled personnel and the necessary equipment differs heavily between countries. A great example of a well-prepared country is Germany, though being criticised in the past about the large number of ICU beds, which turned out to be a big asset during this pandemic. Germany had a relatively high number of ICU beds per 100,000 people and a relatively low number of deaths related to COVID-19.
Approaches by European countries to increase capacity in past months
Other countries were not as prepared for the large inflow of patients and needed to increase capacity fast and in innovative ways. In London a temporary hospital with 4,000 beds was opened in a convention centre for non-critical patients to release some of the pressure on other hospitals. By the time the virus peaked in Spain, regions such as Madrid and northeast Catalonia already tripled their ICU capacity. Furthermore, Spanish hotels turned into recovery rooms and field hospitals were built in sport centres, libraries and exhibition halls.
As exemplified above, several strategies have been undertaken by countries, e.g. Italy, to expand capacity during the pandemic that includes:
- Postponing non-urgent procedures to transform operating rooms into ICU’s (often already equipped with ventilators).
- Upgrading semi-intensive care beds into full intensive care beds (often already equipped with ventilators).
- Using ventilators as efficiently as possible, by putting protocols in place to wean patients off ventilators where possible.
- Creating designated non-intensive care hospitals or temporary recovery hospitals where patients can be transferred when they don’t need ventilation support.
Increasing suitable hospital beds is only part of the problem, as elaborated in the WHO guidance for strengthening the health systems in response to COVID-19. Hospitals need an appropriately skilled workforce, but health workers who are trained for the unique and dynamic critical care are scarce. For example, due to the lack of protective equipment in Italy, many of the healthcare workers got infected too, and some even died. Italy, the United Kingdom, and France are examples of countries that turned to medical students and retired doctors for help. In Italy, for example, 20,000 additional healthcare workers have been hired, including 4,300 physicians and 9,700 nurses, resulting in a total increase of 3.5% in medical staff according to newspaper La Stampa. Moreover, supplies such as ventilators are critical equipment to support the breathing of patients yet are sometimes as scarce as ICU beds.
As healthcare systems were becoming overwhelmed across European cities and states, it forced national authorities to work together, both with their own hospitals and medical staff, as well as with other countries. For example, Paris doubled it ICU capacity, but filled this rapidly. Afterwards, they transferred patients to less saturated regions using high-speed trains, military planes, and helicopters. Some European countries relied heavily on other, sometimes less wealthy, countries. For example, Cuba sent doctors to France, Spain, and Italy and Turkey sent masks, hazmat suits, goggles, and disinfectants to Italy and Spain. The large hospital bed capacity in Germany gave them the opportunities to help critical patients from neighbouring countries, such as the Netherlands.
Preparation for potential second wave
Currently, countries are lifting restrictions, the spread of the virus is slowing down, and the pressure is easing on the healthcare systems. However, there is a concern that, in a couple of weeks or months, the virus will resurface causing new infections and flooding hospitals all over again. This is often referred to as a ‘second wave’. A second wave could appear when containment measures are lifted too quickly, a mutant of the virus appears, and even the colder weather can play a role.
It is difficult to predict the course of a second wave or whether there will be a second wave at all. European countries experienced the last few months how fast the virus can spread and the consequences that it can have for the healthcare system. Efforts are already put to be prepared for a second wave.
In April 2020, the WHO launched the Adapt Surge Planning Tool, which will assist health planners in Europe to prepare for the surge in COVID-19 patients in need of acute care. The tool visualises and estimates the health workforce necessary for acute and intensive care over the course of the pandemic. It can help estimate the number of hospital bed required, predict the days of shortages and provide details on needed human resources. This was helpful for the first peak of the virus and can be a start in preparing for a possible second wave.
To prevent a second wave of infections, governments follow recommendations from experts closely (e.g. by WHO) and support the development of a vaccine. Until we reach a stage where the virus is fully contained, social distancing among other measures are expected to be helpful in preventing a second wave and easing the pressure on healthcare systems.
Looking for more open data related news? Visit the EDP news archive and follow us on Twitter or LinkedIn.